
Articulation Therapy
Articulation Therapy
Articulation therapy refers to targeting specific speech sounds to improve intelligibility. The goals and treatment plan look differently for every individual. Here is a simple guide to articulation therapy for professionals, caregivers, and graduate clinicians.
What are developmental norms for speech sounds?
Speech sounds develop by different ages depending on how they are produced by the ‘articulators’. Articulators include:
- Lips
- Teeth
- Tongue
- Jaw
- Alveolar ridge- gum ridge behind top teeth
- Palate- roof of mouth
- Larynx- voice box
- Nose
- Pharynx- throat
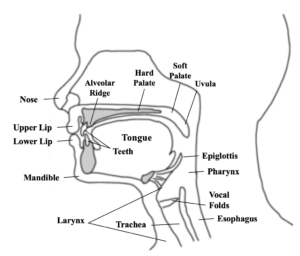
Sounds that are visible and produced with the lips, such as /p/ and /b/, emerge first. This is because it’s easy for children to see how the sound is produced and imitate. Sounds that are produced in the back of the mouth, such as /k/ and /g/, also emerge early in life. The reason for this is that infants spend a lot of time on their backs and gravity helps them learn to use the back of their tongue as they are engaging in vocal play and blowing raspberries. Sounds that are produced in the middle of the mouth are the last to emerge because they are harder to see, therefore harder to imitate, and require a more fine-tuned articulator placement.
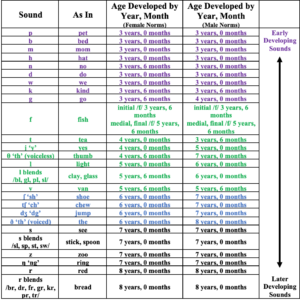
There are several developmental norms for articulation out there. I use the Iowa-Nebraska norms most frequently when determining if speech sound errors are age-appropriate or not:
To determine the impact of articulation errors, a child’s intelligibility level should be considered. Meaning how well they are understood by others. Below are the expected intelligibility levels by age according to Pena-Brooks, Adriana, & Hedge:
- 2 years: Unfamiliar listeners should understand 50% of utterances at the sentence level
- 3 years: Unfamiliar listeners should understand 75% of utterances at the sentence level
- 4 years: Unfamiliar listeners should understand 75-90% of utterances at the sentence level
- 5+ years: Unfamiliar listeners should understand 90-100% of utterances at the sentence level
What should we do if a child says sounds incorrectly?
Find a Speech-Language Pathologist (SLP) to complete a full speech/language evaluation. The SLP will determine if your child’s speech and language skills are age-appropriate or recommend therapy to address a speech sound disorder.
The exact cause of speech sound disorders is unknown but they likely are not linked to one contributing factor. The most common risk factors:
- Recurrent ear infections in early childhood
- A parent or sibling that has/had a speech sound disorder
What will articulation therapy look like?
The most commonly used technique to address speech sounds is what is called the “Traditional Articulation Hierarchy.” Individual sounds are first taught and then practiced in short utterances gradually moving to longer utterances and spontaneous speech. The 7 levels are:
-
Isolation:
First, the client is taught to produce the sound on its own. Depending on the sound, this can take a short amount of time or longer for harder to produce sounds. The SLP will have a bag of tricks to elicit speech sounds using anything from verbal prompts about tongue placement and airflow to tactile cues for reinforcement of tongue and jaw position such as a lollipop or tongue depressor.
-
Syllables:
After the client can produce the sound, it’s time to start pairing the consonant with vowels to form syllables. Syllables are usually the target consonant + vowel (ex. “Sue”) or vowel + target consonant (ex. “Us”).
-
Words:
After syllables, target sounds are then practiced with real words. There are three-word positions to work through initial, medial, and final. This means that the target sound can occur at the beginning of a word (initial position), middle of a word (medial position), and end of a word (final position). Clients may have an easier time producing the target sound in one word position compared to the others. Therefore the word level is usually first addressed using block trials, meaning only one-word position is addressed at a time. Gradually the trials can become random so that all word positions are addressed at once. Another thing to consider at the word level is the number of syllables per word. It’s best to start with one-syllable words and gradually move to two and three-syllable words.
-
Phrases:
Generally, the isolation, syllable, and word levels are a lot of practice and drill and can sometimes take the longest time to master. Once the client has mastered these levels, it’s time to start working on the carryover of the target sound into utterances that gradually increase in length. The first place to start for carryover is at the phrase level, which consists of 1-2 words combined with one word that contains the target sound (2-3 words in total). To keep things simple, use a carrier phrase such as “my” or “I see” and have the client rotate through the target words.
-
Sentences:
After phrases comes sentences, which should be about 5 words in length (including one word with the target sound). Sentences can also be a carrier sentence that the client repeats and rotates through the target word list or they can be unique and change for each target word.
-
Reading:
For clients who can read, reading passages that contain a large quantity of their target sound/s is the next step. Passages should begin with a few sentences and then gradually increase in length.
-
Conversation:
The last and final step into mastering a target sound is to practice spontaneous speech or conversation. Up until now, the client may be showing steady progress as the other levels are structured. It’s normal to see a little regression in sound production when first beginning this level. This level can sometimes take a while since the client is building a new habit to replace their old one of incorrect sound production in conversation in the home, school, and social settings.
View my Articulation Digital Cards HERE.
What if the client continues to have difficulty?
In any of the levels listed above, the client may have more difficulty compared to the others. This is quite normal. Target sounds are impacted by consonants and vowels that both precede and follow them. These are constantly changing as the target sound is used in new words, phrases, and sentences. If a client is having difficulty with a specific word, the SLP can have the client work back down the levels while practicing the target and then work back up.
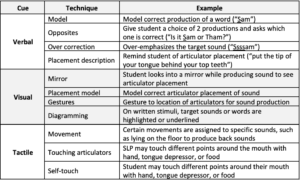
The SLP may also try verbal, visual, or tactile cues to help the client produce or remember the sound. Techniques and examples include:
What can be done at home to help with sound production?
The most important thing for caregivers to do is to model the sound/words correctly at home. You can restate the word to the child while emphasizing the sound they produced incorrectly. Do not imitate what the child is saying. Sometimes adults think it’s cute to imitate how a child mispronounces words and even add it to everyday vocabulary. This will only reinforce their incorrect productions.
The SLP will most likely give homework once the client has mastered the sound and can successfully practice with others. Stick to the homework that is given to avoid working on words or levels that are too difficult for the client and may lead to frustration.
Building the client’s phonological awareness skills (listening skills) will also improve speech production. Ways to build phonological awareness skills are to:
- Play rhyming games: Give the client a word and have them think of as many words, both real and non-sense, that rhyme as they can.
- Practice opposites: Using a list of target words from the SLP, say each word correctly – incorrectly- correctly.
- Be the client: Using a list of target words from the SLP, say some of the words incorrectly and have the client correct you.
- Auditory Bombardment: Read books aloud to the client and point out words that contain their target sound. Exaggerate your production of the sound while saying the words aloud.
In summary, there is no specific timeline or technique for articulation therapy. Each client will progress at his or her own pace. It’s important to be consistent with practice and keep the therapy fun and engaging!
For information on parts of a speech-language evaluation, read my blog post An Oral Periph Exam.
2 Comments